|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Suppurative hand infections
1. Suppurative diseases of the skin and subcutaneous tissues: cutaneous abscess; corn abscess; interphalangeal (commissural) phlegmon; supraaponeurotic phlegmon of the palm. 2. Suppurative diseases of the fascial and interstitial spaces: phlegmon of the mid palmar space; thenar phlegmon; hypothenar phlegmon. 3. Suppurative diseases of the dorsal aspect (dorsum) of the hand: subcutaneous phlegmon. Suppurative diseases of the hands and fingers are among the commonest diseases in ambulatory surgical practice. The development of these acute pyogenic infections is preceded by minor skin injuries: stab wounds, contusions and abrasions. With the aim choosing a rational therapy the period of infection is divided into the initial (serousinfiltrating) and suppurative (purulent-necrotic) stages of the inflammation. The clinical picture of the suppurative hand infection exhibits both general and local features: oedema, hyperemia, pain (fig. 94), increase in body temperature and functional disorders. However, infections of the subcutaneous fatty tissues of the palm are only associated with tenderness on palpation and some amount of smoothening of the palmar folds. Other signs of inflammation (hyperemia, pronounced oedema) are more prominent at the dorsum. Cutaneous felon. In cutaneous panaritium the exudate is located beneath the epidermis and divides it by forming blisters (fig. 95) whose contents can be serous, purulent or hemorrhagic. Cutaneous panaritium can sometimes be associated with high body temperature, regional lymphadenitis and lymphangitis, which is accounted for by the presence of very virulent infections. Subcutaneous felon. This is one of the most commonly encountered hand infections (see fig. 95). It is most often reported at the purulent stage since patients rarely seek medical advice in the early stages of disease. The hallmark of the condition is tenderness at the focus of inflammation. Pain increases gradually, and is of throbbing and pulsating character. Patients normally go about their daily business during the first hours and sometimes even the first days of the disease. Pain, however, increases in intensity and the victims may become uncomfortable and unable to sleep.
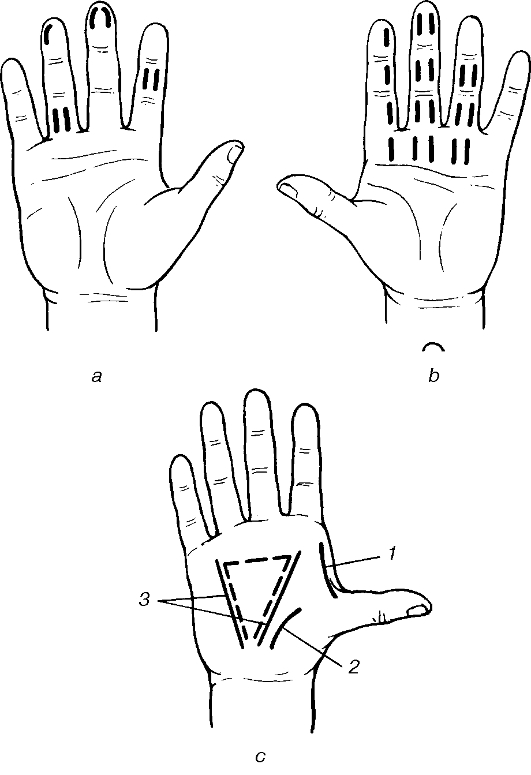
Fig. 94. Zones of tenderness in suppurative hand infections: 1 - osteal felon; 2 - articular felon; 3 - subcutaneous whitflow; 4 - thecal whitflow; 5 - corn palmar abscess; 6 - 1st digital and radial tenobursitis; 7 - 5th digital and ulnar tenobursitis.
Fig. 95. Topography of abscesses in hand infections: 1 - subungual felon; 2 - paronychia; 3, 4 - subungual paronychia; 5 - cutaneous whitflow; 6 - subcutaneous whitflow; 7 - «cuff-link»-type subcutaneous whitflow; 8 -thecal whitflow; 9 - articular felon; 10 - osteal felon; 11 -infection of the distal phalanx; 12 - pandactylitis. Examination of the finger reveals tension in the tissues with the finger folds at the interphalangeal joints leveled out around the focus of infection. Skin hyperemia is not so distinct. Using a blunt probe for methodical and systematic palpation, the most painful area, which corresponds to the location of the pus, can be easily identified. The patient's general condition is bad because of the persistent pain. The connective tissue bands in the subcutaneous layer, which connect the skin to the periosteum, prevent the pus from spreading to the periphery. The tension in these tissue bands causes intensive pain in the finger. The pus in subcutaneous panaritium tends to spread to the deep-lying tissues. Paronychia. This is an inflammation of the areas around the nail fold, associated with tender swellings of the nail fold and hyperemia of the surrounding tissue. Examination reveals the affected nail fold floating over the nail plate (fig. 96, colour inset). Palpation of the edematous area around the affected nail phalanx is tender. The fast rate of spread of the infectious process quickly renders the affected person incapacitated. In certain instances of paronychia the pus can spread to beneath the nail plate dividing it from the lateral or proximal sides. In this way the purulent exudate shows through the divided nail end. Hyponychial felon. This is characterized by the accumulation of pus beneath the nail plate, dividing the latter from the nail bed either along its entire length or at some particular areas. Its presence is noted with the loosening of the nail plate, its fixation to the bed is lost and the nail is only fixed firmly at the proximal ends at the matrixes. The accumulation of pus is visible beneath the nail plate either along its entire length, or in small areas of proximal, lateral or distal portions of the nail bed. Oedema and skin hyperemia are minimal in hyponychial panaritium. The main symptoms are pulsating throbbing pain at the nail phalanx. There is tenderness on palpation or percussion of the nail plate. Articular felon. This type of infection often occurs after injuries to the dorsum, interphalangeal or carpophalangeal aspects where the joints are covered by only a thin layer of soft tissue. Pain during the serous phase of infection is quiet intensive, making the patient feel very uncomfortable and reducing considerably his work input. The inflamed joint assumes a fusiform appearance. Dorsal interphalangeal folds smoothen up. An attempt to bend the finger in the affected joint causes extreme pain. There is a local increase in temperature. Oedema and hyperemia are more pronounced at the dorsal aspects. Puncture of the joint space yields some minimal turbid fluid. If the condition is not treated early and the infection spreads to the connective, cartilage and bony apparatus of the finger, then a pathological motility, and a sensation of crepitus of the cartilaginous articular surfaces of the bones may be evident. Osteal felon. This condition as a rule develops as a secondary process, when the process spreads from the soft tissues of the fingers to the bone, mainly in the case of subcutaneous panaritium. In such cases after the pus has been drained from a subcutaneous panaritium, followed by a brief period of seeming improvement in health, reduction of oedema and pain, recovery does not occur. Pain in the hand becomes dull and nagging, minimal purulent discharge from the wound persists and sometimes even with small particles of bony sequestra. The finger gets clubbed and puffy and tender on palpation. Signs of bone destruction on the X-rays are apparent only towards the end of the 2nd - the beginning of the 3rd week. Surgery should be performed based on the clinical presentation without having to wait for clear-cut X-ray features of bone destruction. Tendinous felon. In some cases subcutaneous felon may trigger tendovaginitis as a result of spread of the infection to the tendons and the tendon sheaths of the flexor digitorium muscles. The patient's general condition deteriorates, a shooting and throbbing pain spreads to the whole finger, evenly spread oedema with smoothening of the skin folds at the interphalangeal joints is present. The finger appears to be sausage-like and is slightly bent in this position, with the result that the tension on the tendons is relieved and the pain reduced. Attempt to extend the finger causes extreme pain. Palpation with a probe along the tendon sheath is very painful. The above signs as well as the clinical presentations help to establish the diagnosis of tendon panaritium (tendovaginitis). Delay in the surgical treatment of tendovaginitis is very dangerous, because once the blood supply to the tendon is cut due to the pressure of the exudates on the mesotendon vessels, the tendon is rapidly necrotized. Pandactilitis. This is a suppurative inflammation of all the finger tissues. Pandactilitis is a serious infection associated with severe intoxication (headache, elevated body temperature), regional lymphangitis; cubital and axillary lymphadenitis. Peripheral blood picture shows the changes typical for acute suppurative inflammations. Pandactilitis develops gradually. It is caused by the virulent infectious contamination through a hand injury. It can also result from a simple panaritium, especially the subcutaneous one. As pandactilitis develops, pain gradually increases in intensity, and the sick person experiences an intense, excruciating and distending pain. The oedematous finger is of a bluish-violet colour. The infection can be either of a dry or wet necrosis. The discharge from the suppurative fistula or the postoperative wound is scanty pus; granulation is grey and dead (see fig. 96, colour inset). Palpation is tender all over the involved area and an attempt to move the finger may cause extreme pain. The patient's condition deteriorates, the temperature of the body increases, oedema and hyperemia of tissues increase and extend in the proximal direction. It is only an immediate surgical intervention that can stop the progression of the suppurative inflammatory process. Hand phlegmon (fig. 97). The local signs of hand phlegmon are: tissue oedema and hyperemia, hand dysfunction, increase in the local temperature and tenderness on palpation. Phlegmon of the ball of thumb (thenar eminence). This is accompanied by an extreme oedema of the thenar and the radial end of the dorsum of the hand. Severe pain on palpation, tense tissues, limitations in the mobility of the oedematous thenar tissues, smoothening of the palmar folds are all characteristic symptoms of thenar phlegmon. The purulent exudates can sometimes also spread along the first interosteal muscles on the dorsum. In other cases the connective tissue barriers that divide the thenar from the mid palmar space disintegrate as a result of the suppurative process causing phlegmon of the mid palmar cavity. Phlegmon of the hypothenar is often accompanied by mild intoxication. Minimal oedema, hyperemia and tension in the tissues, tenderness on palpation over the hypothenar and an increase in pain upon moving the little finger are the characteristic features. Commissural phlegmon is localized at the distal part of the palm. The entry points of infection are usually deep skin fissures and skin callosity over the area of the 2nd-4th carpophalangeal joints of the palm. This phlegmon is also known as corn abscess. Phlegmons are associated with extreme pain, oedema on both sides of the hand. Fingers adjacent to the area of infection are somewhat spread apart and bent in their interphalangeal joints; extension is painful as a result of the tension on the inflamed palmar aponeurosis. It is possible for the pus to spread directly through the oval fissure of the aponeurosis to the dorsal surface of the hand, involving in the process the tendons of the deep flexors, which are situated very closely. The spread of infection can also occur in the proximal direction along the canals of the vermiform muscles, involving in the inflammation process the mid palmar space (fig. 98).
Fig. 97. Topography of phlegmon in palmar and dorsal hand infections: 1 - subcutaneous; 2 - palmar supratendinous; 3 - subtendinous; 4 - thenar; 5 - hypothenar; 6 - dorsal subcutaneous; 7 - dorsal subfascial. Phlegmons of the mid palmar space are associated with the accumulation of pus in between the palmar aponeurosis and the thin fascial sheath covering tendons of the flexor digitorium or between the fascia covering the palmar sides of the interosteal muscles and the posterior surface of the tendons of the long flexor digitorium. The disease is accompanied by pronounced intoxication, high body temperature, headache, as well as changes in the peripheral blood picture. Examination of the hand reveals a swelling in the central palmar area, the skin is tense, skin folds are smooth and fluctuation is not possible to elicit. Palpation over the inflamed region may cause extreme pain. The dorsum of the hand is very oedematous. The 2nd-5thfingers are slightly bent in the interphalangeal joints, attempts at passive or active movement cause extreme stretching of the inflamed palmar aponeurosis, which results in pain increase. Delayed or irrational treatment of mid palmar space phlegmon may entail a complication with the abscess bursting into the thenar fissure and the pus spreading along the canals of the vermiform muscles on the dorsum. Crossed or U-form phlegmon is the most severe form of suppurative hand inflammation. The disease results from a purulent tendovaginitis of the 1st or 5th finger with a spread of the purulent exudates to radial and ulna synovial sacs. U - form phlegmon is accompanied by pronounced intoxication, high body temperature, headache, as well as body weakness. The hand is oedematous, bluish-violet in colour and palpation is extremely tender. The fingers are bent towards the palm, active movement is absent. Attempts at passive movement may cause extreme pain. By means of palpation the area of extreme tenderness is found to be around the projections of the 1st and 5th tendons and in the proximal parts of the hand, that is, at the site of the blunt ends of the radius and ulna synovial sacs. When the pus bursts into Pirogoff's space, diffuse tenderness and oedema of the distal parts of the forearm may result. The suppurative inflammatory process can spread to the mid palmar space, fissures of the thenar or hypothenar in the case of tenobursitis of the 1st and 5th fingers. Subsequently the pus spreads through the canals of the vermiform muscles to the dorsum of the hand to form an extensive purulent-necrotic area. Even with favourable resolution of U-type phlegmon the distant postoperative period is associated with limitations in the functions of the hand. Hence, it is very important to have a timely diagnosis and surgical treatment of this condition. In subcutaneous phlegmon of the dorsum of the hand tissue oedema and hyperemia are of diffuse nature, and it is difficult to determine the demarcation line of the infection. Thorough palpation can help to assess the area of tissue softening. Subaponeurotic phlegmon of the dorsum of the hand occurs as a result of infection penetrating deep under the aponeurosis in the case of stab wounds.
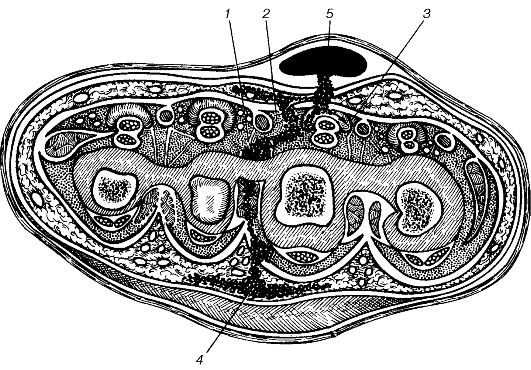
Fig. 98. Topography of suppuration in corn abscesses (frontal view): 1 - interosseous fissure; 2 - mid-palmar space; 3 - tendon sheaths; 4 - dorsal hand fat; 5 - corn abscess. In this kind of phlegmon a firm induration is observed which is associated with oedema and hyperemia of the dorsum. Subcutaneous phlegmon also occurs, as a rule, secondary to damage to the skin covering of the dorsum of the hand. In suppurative affection of the palm there can be transmission of the infection to the dorsum through the lymphatic vessels or through the canals of the vermiform muscles. In such situations oedema of the dorsum that is normally present in palmar lesions is accompanied by skin hyperemia, and the appearance of a diffusely tender area on palpation. Furuncles and carbuncles of the hand. Oedema, hyperemia and extreme tenderness on palpating the dorsal aspects of the finger or hand, and the presence of a necrotic core are the symptoms of furuncles. In the case of carbuncles these symptoms are more acute, there being several necrotic cores; the patient's general condition deteriorates and the features of intoxication are more pronounced (headache, weakness, rise in body temperature), regional lymphadenitis and lymphangitis. Treatment. During the serousinfiltration stage of the inflammation alcohol compress, baths, electrophoresis with trypsin, chemotrypsin, antibiotic therapy including the regional intravenous infusions of antibiotics and ultraviolet irradiation therapy are used. The first sleepless night as well as severe tenderness on pressing the affected area, the appearance of a firm swelling in the soft areas of the palm, oedema of the surrounding tissues are indications for surgery. In subcutaneous panaritium of the distal and middle phalanx, hyponychial panaritium (subungual) and paronychia, surgery can be performed without pain by using the block anesthesia method of Oberst-Lukashevich. A tourniquet applied at the base of the finger helps to perform the operation without bleeding, which allows for a good orientation in the wound and cleansing it of all the necrotic tissues. In severe forms of panaritium (tendinous, pandactilitis), phlegmon of the hand surgery is performed under conduction local anesthesia. In very severe phlegmon of the hand and phlegmon of Pirogoff's space, surgery is performed under intravenous general anesthesia. Operations on the hand should be done using ophthalmology instruments (scalpels and sharpedged scissors). These instruments allow for adequate incisions, easy manipulations in the wound, gentle handling of the viable tissues and can effectively remove all the necrotic tissues in the wound.
Fig. 99. Lateral linear incisions: digital in subcutaneous (a) and subtendineous (b) whitflow; palmar in phlegmon (c); 1, 2 - dissection of thenar phlegmon; 3 - dissection of the palmar space. The projection of the palmar space is dotted. Depending on the extent of the purulent process single or double linear incisions are made on the sides of the finger (fig. 99). With the exception of cutaneous, hyponychial and cutaneous abscesses of the palm, all operations are completed by wound drainage. For this purpose use is made of rubber fenestrated drainage tubes are used, which allows for periodic or constant irrigation of the wounds with solutions of antiseptics or proteolytic enzymes and this in turn facilitates quick removal of the pus, reduces pain, enhances the shedding of necrotic tissues and a faster healing process (fig. 100). In cutaneous and hyponychial panaritium only the split (disintegrated) part of the epidermis, or the nail plate is incised, the wound is washed with a 3% solution of hydrogen peroxide and the surrounding skin is cleaned with alcohol solution (fig. 101). Incision and drainage of tendon sheaths is done by single (one sided) or parallel (on both sides) lateral linear incisions on the middle and proximal phalanges. Drainage of the tendon sheaths is done by the rubber fenestrated drainage tubes, placed perpendicularly above the tendons so as not to damage the mesotendon.
Fig. 100. Fenestrated drainage: a - general view; b - insertion of the drain; c - drainage of the wound with a tube; d - extraction of the drain.
Fig. 101. Surgeries for nail plate involvement: a - trephination of the nail plate (1, 2); b - wedge-shaped incision of the nail plate followed by removal of a foreign body (1, 2); c - removal of the nail plate (1, 2); d - surgery for nail wall and base involvement: 1 - cutaneous incision; 2, 3 -nail wall and base incision; 4 - the nail post surgery. In case of panaritium involving the bones and joints, double lateral linear incisions are made, the purulent necrotic cavities are opened and cleansed. Necrotic tissues and sequestra are evacuated, the affected bones are resected and the wound drained with fenestrated drainage tubes. To prevent generalized infection and to eliminate the purulent foci during pandactilitis of the 1st-5th fingers when other forms of treatment have failed, exarticulation of the finger is done as an ultimate measure. In the case of pandactilitis of the 1st finger (the thumb) the surgeon should always hesitate to perform this type of operation since even if the thumb loses its extensor-flexor qualities it still maintains the function of opposition without which the patient becomes disabled. In performing operations in the case of palmar phlegmon one has to consider the fact that there is always oedema at the dorsum. Even in the presence of pronounced oedema at the dorsum one should never make an incision over this area before the presence of suppuration in the fingers and palm has been confirmed. However, if after an incision and drainage of a palmar or finger abscess the dorsum continues to swell, becomes more hyperemic and firmer, then there is good reason to think that the contralateral oedema has become suppurative. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 195; Нарушение авторского права страницы